|
||
The Male Climacteric:
|

When synthetic testosterone became available in the mid-1930s, and when the Nobel Prize was awarded for that synthesis in 1939, interest in the new compound---both scientific and commercial---increased. Among those studying effects of the new hormone were Carl Heller and Gordon Myers, Wayne University endocrinologists working at the Detroit Receiving Hospital. Among the pharmaceutical firms seeking to advance the cause of their product was the Schering Corp, which had backed Butenandt in the original synthesis of testosterone. Thus did Heller and Myers receive funding from Schering to study the effects of its drug testosterone propionate in the 'male climacteric.' Although not the first to administer synthetic testosterone, Heller and Myers performed one of the most thorough, systematic researches of the time. Their stated mission was to determine if 'male climacteric' has an organic basis and is a true clinical entity.
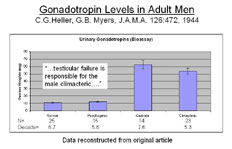
Normal men and men with psychogenic impotency were found to have normal levels of gonadotropins, while castrates and men with 'climacteric' were found to show markedly elevated gonadotropin levels. In some men, testis biopsy was used to confirm a diagnosis of gonadal failure.
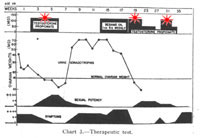
Heller and Myers summarized their findings as follows: "The diagnosis of the male climacteric was established in 23 cases by the finding of pronounced elevation in gonadotropic hormone excretion, comparable quantitatively to that occurring in castrates. This was corroborated in all 8 cases subject to (testicular) biopsy by histologic evidence of testicular atrophy and degeneration. The diagnosis was further supported in all 20 cases treated by specific response to a therapeutic test with androgens. A clear cut differentiation of the male climacteric from psychogenic impotence was made by urine gonadotropic assays, which were decidedly elevated in the former group and normal in the latter. A simple therapeutic test is helpful in distinguishing between these two conditions. The symptomatology of the male climacteric is different from that of psychoneurosis and psychogenic impotence. Satisfactory therapeutic results were obtained by intramuscular injections of testosterone propionate and by implantation of testosterone pellets, but not by the oral or sublingual administration of methyl testosterone." |
||||
|
|